Pharmacists. We’re the experts in medicines, right? But what does that mean in practice, and how does our conduct in the community (retail…) sector fit with the rest of the healthcare team and the direction in which it travels?
This is something spoken about on Twitter before, and a topic I’ve often pondered as both a locum and customer at community pharmacy. To help frame this some more, it’s my absolute pleasure to be able to post an article by a crackin’-good pharmacist which was recently published in Medical Writing. For you referencing geeks out there, it’s: Johnson, H. Selling Evidence over the counter: Do community pharmacists engage with evidence-based medicine? Medical Writing 2013; 22(4): 275-278.
Read it, consider it and let me know what you think with a comment or tweet as ever please. But most of all – enjoy!

From the author:
“A while ago, I was asked to write an article by Adam Jacobs (@dianthusmed), who was guest editing an issue of Medical Writing. The theme for the issue was Good Pharma.
I had intended to write something about how different the sort of evidence base community pharmacists have access to differs to the sorts of evidence (or lack of) that accompanies complementary and alternative medicine. But, during my literature searches for the article, I was taken in a very different direction. I started wondering about how and why community pharmacists engage with evidence-based medicine (EBM). I often think that, in discussions about it, the practicalities of life as a busy front-line pharmacist can be forgotten. I wanted to see what the evidence had to say on the matter, and this is the resulting article.”
Selling evidence over the counter: Do community pharmacists engage with evidence-based medicine?
Traditionally, products sold over the counter (OTC) in a pharmacy may have been guided more by commercial gain than rational, evidence-based medicine (EBM). Even those products that are licensed may not have a robust evidence base for their effectiveness. Irrational combination products, cough medicines, and unproven complementary medicines line the shelves of most stores, leading some prominent promoters of good science to recently criticise pharmacy as a ‘quack trade’.1
As the role of the pharmacist evolves, it is becoming more and more imperative for the profession to distance itself from quackery and embrace EBM. This is particularly important in the face of deregulation of prescription-only medicines, the potential for self-selection of pharmacy medicines by patients, and a general public that is increasingly willing to take responsibility for its own healthcare.2
The cornerstone of EBM is the ability to locate, appraise, understand, and communicate clinical evidence. Pharmacists often act as the front-line interface between the patient and the healthcare service and as such require the skills to translate complex statistical health information into language which patients are likely to understand and engage with.3
Opportunities for EBM in the community pharmacy
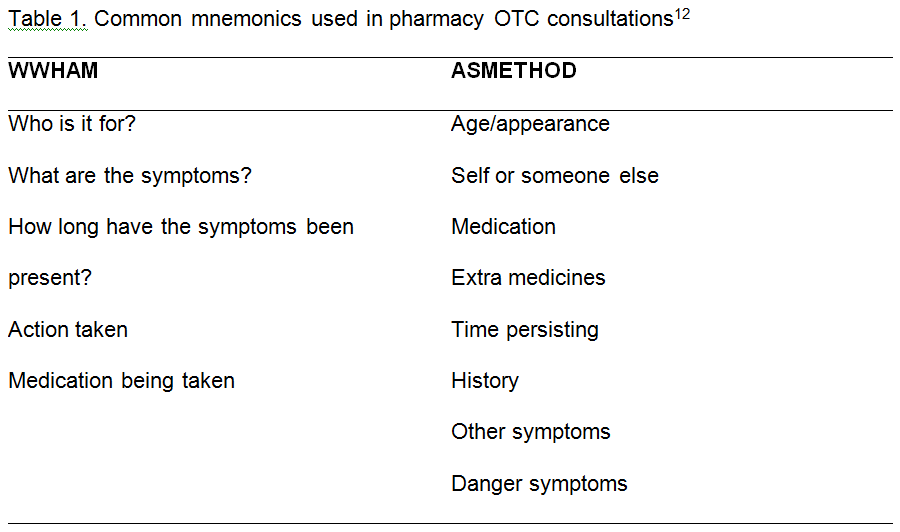
An effective OTC encounter in a pharmacy is a stepwise, logical process of elimination, using good questioning and knowledge to narrow the available products suitable for an individual patient. The first step involves the use of careful, structured questions, usually following a mnemonic (see Table 1), to establish the symptoms and check the diagnosis. Symptoms which require referral are identified and patients directed to appropriate services where required. Once the diagnosis is identified, the range of OTC products available to treat it will be borne in mind by the pharmacist. Knowledge gained from questioning about the patient’s medical history and drug history is used to eliminate any products which are inappropriate for the individual patient due to cautions, contra-indications, or drug interactions. The pharmacist may then recommend a product based on a number of factors. Counselling points on how to use the product effectively and safely should then be conveyed to the patient.

As some of the most easily accessible health care professionals, community pharmacists often deal with patients presenting with health- and medicines-related questions, which may be prompted by sensationalist media reporting or information gathered from friends, family, or the Internet. There are therefore clear opportunities within daily community pharmacy to utilise clinical trial evidence in accordance with the principles of EBM.
The evidence for a lack of evidence
A survey conducted in 2005 amongst pharmacists from all sectors in Illinois by Burkiewicz and Zgarrick found that 90% of 323 pharmacists held positive attitudes towards EBM.4 In a more recent survey of community pharmacists in Northern Ireland conducted by Hanna and Hughes, 88.3% of 205 community pharmacists stated that they were familiar with the concept of evidence-based practice.2 This is indicative of a profession that understands the underlying concepts of EBM.
In spite of these studies, there is an overall lack of robust evidence community pharmacists’ attitudes and uptake of EBM, and the currently published evidence is limited by small sample sizes and methodological flaws. However, the qualitative studies which do exist offer an interesting insight into the considerations when selecting an OTC preparation.
Hanna and Hughes conducted a series of surveys into pharmacists’ attitudes to OTC sales.2 They found that the over-arching concern when selecting a product was patient safety, with 91.8% of pharmacists agreeing or strongly agreeing that safety was their main concern. Effectiveness of the product was of secondary interest. Pharmacists cited patient and colleague feedback, along with personal or family use, as the most common methods to determine a product’s effectiveness, with clinical trial data appearing to be a less important consideration. This would seem to be at odds with the principles of EBM, and suggests that while pharmacists are broadly in favour of EBM, their ability to use it in their everyday job is limited. Over 60% of respondents agreed that evidence-based practice is more difficult for community pharmacists compared to other healthcare professionals.2
In May 2013, the consumer magazine Which? performed an undercover investigation of the quality of advice given in a sample of 122 community pharmacies in the UK. The report found that unsatisfactory advice was given by pharmacy staff in 43% of visits.5 While this report has been widely criticised due to its small sample size,6 it may be indicative of a wider problem which may be improved by increased uptake of EBM. Which? also investigated the evidence for claims made for a variety of healthcare products, and has published a list of ten popular and widely available pharmacy products for which no good evidence of benefit exists. This includes well known brands such as Benylin and Covonia cough medicines, Bach’s Rescue Remedy, Bio-Oil, and Boots Cold and Flu Tablets.7
Reasons for the lack of EBM uptake
In the 2005 study by Burkiewicz and Zgarrick,4 45% of all pharmacists cited lack of time as the main factor limiting their ability to practice EBM. In a community pharmacy setting, the proportion is likely to be even greater, given the fast-paced, unpredictable nature of the retail environment.4 Constant interruptions and juggling many tasks whilst maintaining an open, appointment-free approach to healthcare can lead to a lack of time available for the pharmacist to read and interpret clinical data.
Community pharmacies can be under-resourced to effectively practice EBM, while trusted medical information resources such as Micromedex and Medicines Complete may be too expensive for the average community pharmacy to feasibly access, and can be difficult to navigate in the community pharmacy environment. With the delivery of advanced clinical services such as Medicines Use Reviews – an initiative to improve medicines adherence in the UK by providing support to patients with long-term conditions who are taking multiple medicines8 – along with an ever-increasing dispensing workload, the pressures on a community pharmacist’s time are vast and many.9
The availability of new OTC products and the deregulation of prescription-only medicines can lead to an overwhelming amount of extra training and research for a community pharmacist, on top of their usual daily workload. At present, OTC training tends to take the form of industry-sponsored training packs aimed at enabling community pharmacy staff to sell new products. In my experience, these training packs tend not to address any shortcomings in clinical evidence or proof of benefit, but instead focus more on practical selling points. Whilst they may be adequate to allow pharmacy staff to safely sell a product OTC, they do not always include enough information to allow a pharmacist to make an unbiased, evidence-based assessment of a new product. Moreover, in Hanna and Hughes’ study, only 38% of community pharmacists agreed that they knew how to perform a literature review and critically appraise research papers.2 This highlights a gap in the knowledge of community pharmacists and an important training need. Whilst critical appraisal is covered in pharmacy degree courses and pre-registration training, it may not be used often enough in everyday practice to allow community pharmacists to maintain and hone their skills sufficiently.
Patients appear more likely to rely on personal experience or anecdotal evidence than robust clinical trial evidence when choosing an OTC product, and seem on the whole ambivalent about the need for evidence of effectiveness.10 This, coupled with advertising and the policy in the retail environment that the ‘customer is always right’, means that patients may be unresponsive to messages about lack of evidence from the pharmacist. In an Australian qualitative study, pharmacists reported that advertisements for OTC medicines opposed their professional advice, leading to a sense of disempowerment.11 In the face of consistent rejection of scientific, evidence-based advice, it may be understandable that many pharmacists give up attempting to convey such information.
Solutions
Somewhat alarmingly, Hanna and Hughes2 found that only 23.9% of community pharmacists in their survey were familiar with the work of the Cochrane Collaboration, one of the world’s foremost independent organisations for the dissemination of information about the effects of healthcare interventions. Improving community pharmacists’ awareness of (and access to) reliable sources of medicines information is crucial to improving uptake of EBM in the sector. Pharmacists may not have the time or skills to interpret clinical trial data themselves, so need to have access to robust, concise resources from organisations skilled in the interpretation of evidence. Primary care guidelines such as the Clinical Knowledge Summaries provided by NICE (the National Institute for Health and Care Excellence) in the UK and the guidelines provided by Patient.co.uk can be helpful resources for dealing with minor ailments, but there is a lack of high-quality, independent guidelines for OTC medicines.
Greater collaboration between the pharmaceutical industry and accredited pharmacy training providers may be one solution. An independent review process similar to peer review, but tailored to OTC needs, could be implemented to ensure that any potential biases in industry-sponsored training packs for community pharmacy are reduced. The standardisation of such packs, and inclusion of information on clinical data and its limitations, may improve the ability of pharmacists to make evidence-based decisions.
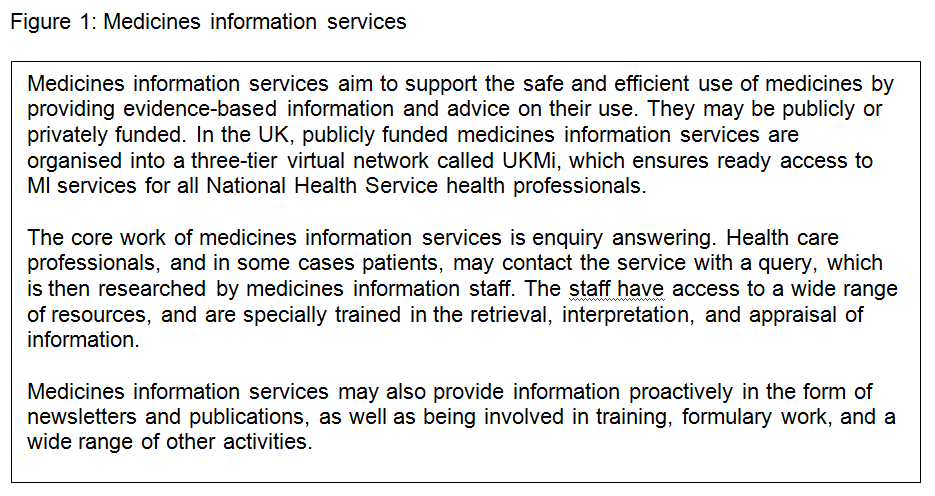
Greater awareness and utilisation of medicines information services (see Figure 1) amongst community pharmacists may be helpful, as these provide a rapid and efficient evidence-based enquiry answering service, allowing community pharmacists to use their time to deliver other services. Staff in medicines information centres are specially trained in the retrieval, interpretation, and appraisal of evidence and can act as a go-between to interpret clinical trial data and apply it to a clinical situation.
There is a clear need for independent training on critical thinking and appraisal skills that is tailored specifically towards community pharmacists. The ability to disseminate complex safety and effectiveness data to patients is a valuable skill that the pharmacy profession could focus on. Questions remain about how best to close the gap between patients’ reliance on advertising and anecdotes and more reliable clinical trial evidence, and any future research in this area will be extremely valuable.

Selling honestly: a personal perspective
I worked as a community pharmacist for many years, and can identify with the use of patient feedback and personal use as the main means of informing OTC product selection. Bombardment with information about new products, along with the highly pressured and stressful job of managing a pharmacy day to day, can be so overwhelming that it can be virtually impossible to keep up with emerging evidence. It becomes easier to rely on more immediate, passive methods of differentiating between products than evidence appraisal.
After moving into a job in the medicines information field, I have improved my skills in finding, appraising, and communicating complex trial information. When undertaking locum shifts in community pharmacy, I have found that this in turn improves and informs my ability to advise OTC. Having more confidence to seek out and question evidence, as well as encouraging critical thinking and evidence communication, allows me to improve an engaged patient’s ability to make an informed choice. I have found patients to be variably receptive to this, with reactions ranging from gratitude, satisfaction, and engagement, through to impatience and, rarely, anger. For the most part, I have found that being honest about the lack of evidence for OTC products increases trust, as patients can see that I am not there primarily for commercial gain, but instead to provide them with good-quality health and medicines advice.
Conclusion
Community pharmacy has an inherent conflict of interest, given its situation as both a retail outlet and a professional healthcare service. Commercial interests may have traditionally outweighed the need for high-quality, evidence-based OTC advice, but a sea change is required to ensure the profession remains a respected part of the wider healthcare community. Other aspects of the healthcare system (and pharmacy) are adopting and implementing EBM, and there is an increased focus on the importance of clinical trial data in the health and popular media following the AllTrials petition (an initiative led by Ben Goldacre, and various other groups, which is calling for all past and present clinical trials to be registered and their results reported). This in turn is exposing the gap between reliable, robust evidence of benefit and how OTC products are currently being sold. Improving understanding of the importance of clinical trial data amongst community pharmacists will be a key step in converting pharmacy from a quack profession into what could more comfortably be considered ‘good pharma’.
References
1. @lecanardnoir 2013. ‘@bengoldacre the unspoken problem is that by any reasonable criteria, pharmacy is a quack trade. It pains me to say.’ Twitter; 2013 May 24 [cited 2013 Aug 19]. Available from: https://twitter.com/lecanardnoir/status/337872315666808832.
2. Hanna L, Hughes C. Pharmacists’ attitudes towards an evidence-based approach for over-the-counter medication. Int J Clin Pharm. 2012;34(1):63-71.
3. Davidson J, Valuck R, Moore G. Evidence-Based Medicine in the Pharmacy. Patient Safety and Quality Healthcare; 2006 [cited 2013 Aug 19]. Available from: http://www.psqh.com/marapr06/ebm.html
4. Burkiewicz J. Evidence-based practice by pharmacists: Utilization and barriers. Ann Pharmacother. 2005;39(7):1214-1219.
5. Can you trust your local pharmacy’s advice? London: Which.co.uk; 2013 May 20 [cited 2013 Aug 19]. Available from: http://www.which.co.uk/news/2013/05/can-you-trust-your-local-pharmacys-advice-319886/.
6. Gregory J. The Which? Scenarios: What would you have done? Chemist and Druggist; 2013 [cited 2013 Aug 19]. Available from: http://www.chemistanddruggist.co.uk/feature-content/-/article_display_list/15729377/the-which-scenarios-what-would-you-have-done.
7. 10 health products you don’t need. London: Which.co.uk; 2012 [cited 2013 Aug 19]. Available from: http://www.which.co.uk/home-and-garden/bathroom-and-personal-care/guides/10-health-products-you-dont-need/.
8. NHS Community Pharmacy Services – a summary. London: Pharmaceutical Services Negotiating Committee; 2013 Jul [Cited on 19/08/2013]. Available from: http://psnc.org.uk/wp-content/uploads/2013/08/CPCF-summary-July-2013.pdf.
9. Gregory J. Dispensing workload in England rockets 62 per cent over decade. Chemist and Druggist; 2013 [cited 2013 Aug 19] Available from: http://www.chemistanddruggist.co.uk/news-content/-/article_display_list/16053812/dispensing-workload-in-england-rockets-62-per-cent-over-decade.
10. Hanna L, Hughes C. Public’s views on making decisions about over-the-counter medication and their attitudes towards evidence of effectiveness: a cross-sectional questionnaire study. Patient Educ Couns. 2011;83(3):345-351.
11. Chaar B, Kwong K. Direct-to-consumer advertising: Australian pharmacists’ experiences with non-prescription medicines. Int J Pharm Pract. 2010;18(1):43-50.
12. ResourcePharm. Pharmacy Mnemonics: WWHAM, ASMETHOD, ENCORE, and SIT DOWN SIR. 4Pharm Ltd. [cited 2013 Aug 19]. Available from: http://www.resourcepharm.com/pre-reg-pharmacist/pharmacy-mnemonics.html.


![IMG_20150920_091240[1]](https://aptaim.net/wp-content/uploads/2015/10/img_20150920_0912401.jpg?w=300&h=225)